Transesophageal echocardiography is a routine procedure attached to an unusually fragmented code set. The TEE CPT code family splits a single exam into components, keeps separate codes for congenital anatomy, carves monitoring out of the diagnostic codes entirely, and reserves one code, 93355, for guidance of structural heart procedures. Selecting the wrong branch produces either an underpayment or a denial that reads “bundled into the primary procedure.” This guide covers each code, the two pairings that generate the most questions (TEE with cardioversion and TEE with anesthesia), and the payer rules that decide whether a claim survives.
How the core TEE CPT codes are organized
CPT structures diagnostic TEE around two questions. Did the physician perform the entire study or only a piece of it? And was the exam performed for acquired disease or for congenital cardiac anomalies?
| Code | What it reports |
| 93312 | Complete 2D TEE: probe placement, image acquisition, interpretation, and report |
| 93313 | Placement of the transesophageal probe only |
| 93314 | Image acquisition plus interpretation and report, without probe placement |
| 93315 | Complete TEE for congenital cardiac anomalies |
| 93316 | Probe placement only, congenital study |
| 93317 | Image acquisition, interpretation, and report, congenital study |
93312 is the default whenever one physician places the probe, obtains the images, interprets them, and signs a report. The component codes exist for split work. The American College of Emergency Physicians, in a January 2022 guidance piece from its ultrasound section, describes a common split: an emergency physician places the probe during resuscitation and reports 93313, while a cardiologist acquires and interprets the images and reports 93314. ACEP adds that the two physicians generally need to belong to separate billing groups or specialties for both claims to pay.
Two smaller details come up constantly. There is no limited TEE code, so ACEP suggests modifier 52 (reduced services) for an abbreviated study, with the caveat that it lowers payment. And when the hospital owns the probe and the echo machine, the physician reports only the professional component by appending modifier 26.
Whichever code applies, the report has to meet CPT’s echocardiography standard: an interpretation of all information obtained, documentation of clinically relevant findings with quantitative measurements, a description of any abnormality, and images archived for later review. A study that skips these elements is not separately reportable at all.
The 93315 CPT code description covers the complete congenital study, with 93316 and 93317 as its probe-placement and interpretation components. National Government Services, the Medicare contractor whose billing article A52868 governs TEE in its jurisdictions, reserves 93315 through 93317 strictly for congenital anomalies.
93318 CPT code description: monitoring is a different service
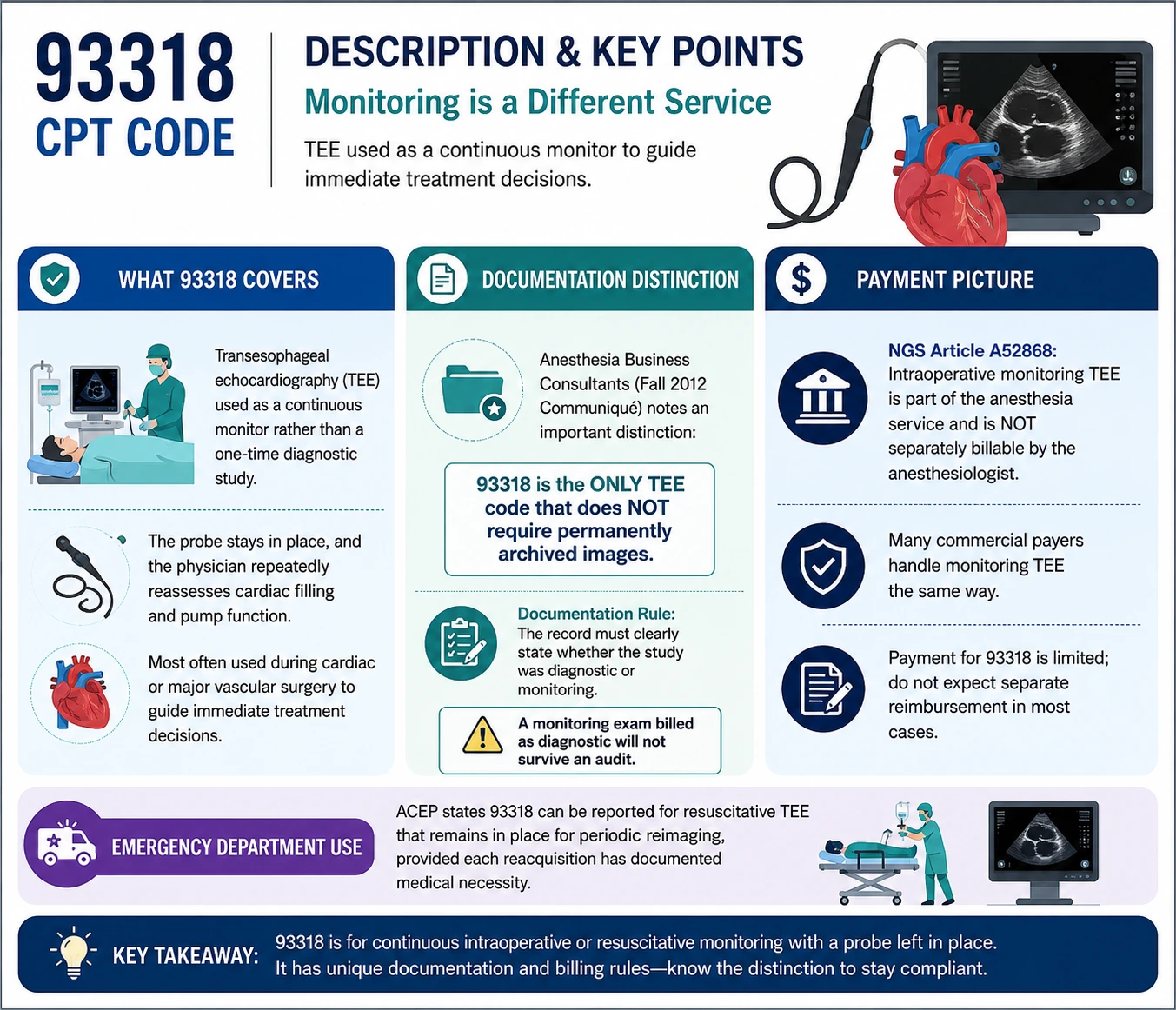
The 93318 CPT code description covers TEE used as a continuous monitor rather than a one-time diagnostic study. The probe stays in place, and the physician repeatedly reassesses cardiac filling and pump function to steer immediate treatment decisions, most often during cardiac or major vascular surgery. Anesthesia Business Consultants, in a Fall 2012 Communiqué article that remains a standard reference on TEE documentation, points out the code’s odd distinction: 93318 is the only TEE code that does not require permanently archived images.
The payment picture is thin. NGS article A52868 states that intraoperative monitoring TEE is part of the anesthesia service and is not separately billable by the anesthesiologist, and many commercial payers handle monitoring TEE the same way. A documentation rule follows directly from this: the record must state whether the study was diagnostic or monitoring. A monitoring exam billed as diagnostic will not survive an audit.
Emergency departments have found one narrow, legitimate use. ACEP describes reporting 93318 when a resuscitative TEE stays in place for periodic reimaging, provided each reacquisition has documented medical necessity.
93355 CPT code: structural heart guidance has its own rules
The AMA added the 93355 CPT code in 2015 for TEE guidance of transcatheter structural interventions: TAVR, transcatheter mitral repair, left atrial appendage occlusion, paravalvular leak repair, and ventricular septal defect closure, among others. The code is deliberately all-inclusive. It covers peri-procedural and intra-procedural imaging, quantitative measurements, the diagnostic TEE itself, ultrasound contrast, spectral and color flow Doppler, and 3D. Nothing from 76376, 76377, or the 93312 through 93325 range may be reported with it.
Three restrictions catch practices off guard:
- 93355 is reported once per intervention, however long the case runs.
- Only a physician who is not performing the intervention may report it.
- Medicare’s National Correct Coding Initiative bundles 93355 into both the interventionalist’s service and the anesthesia service, a point Anesthesia Business Consultants stressed in a March 2020 client alert. In practice, a separately billing imaging physician, usually a cardiologist, is the only one who gets paid for it.
When CMS first valued the code for 2015, it assigned 6.38 total RVUs, about $228 at that year’s national rate. The code’s structure is now under review. Cardiovascular Business reported in October 2025 that the American Society of Echocardiography is drafting a proposal to split interventional echo into procedure-specific codes. ASE president David H. Wiener argued that funneling TAVR, mitral, and tricuspid guidance through a single code makes CMS see “an explosion of imaging” when the volume simply tracks the growth of structural heart programs.
CPT code for TEE with cardioversion
The correct CPT code for TEE with cardioversion is actually two codes. The cardioversion CPT code is 92960 for elective external synchronized cardioversion (92961 for internal), and the pre-procedure TEE is reported separately, usually with 93312. These are distinct services, and both are payable in the same session when both are documented.
Clinical guidelines drive the volume here. Practice standards call for TEE to exclude left atrial appendage thrombus before cardioverting a patient whose atrial fibrillation has lasted 48 hours or longer, or an unknown duration, without three weeks of documented therapeutic anticoagulation. The 2023 ACC/AHA/ACCP/HRS atrial fibrillation guideline permits skipping the TEE in non-anticoagulated patients only as a weak class 2b option, limited to a CHA2DS2-VASc score of 0 to 1 and symptom duration under 12 hours. The exam earns its keep: a 2022 analysis of 512 consecutive pre-cardioversion TEE studies at a high-volume electrophysiology center found appendage thrombus in 3.7 percent of exams, each one a cancelled shock and a changed treatment plan.
The billing details worth memorizing:
- Report one unit of 92960 per cardioversion attempt, regardless of how many shocks were delivered, per ACEP’s reimbursement FAQ.
- ECGs performed before or during the cardioversion are bundled into 92960. A medically necessary post-procedure ECG can be reported with modifier 59.
- 92960 never applies to defibrillation during an arrest. That work belongs to CPR (92950) or critical care time.
- 92961 carries a “separate procedure” designation, so it is not reportable with a catheterization or EP study performed through the same access.
- If the TEE finds a clot and the shock is cancelled, the TEE remains fully billable on its own.
One frequency note: NGS permits repeat pre-cardioversion TEE for repeat episodes of atrial fibrillation or flutter. Repeats outside that pattern require documentation of a genuine change in the patient’s condition.
CPT code for TEE with anesthesia and sedation
There is no single CPT code for TEE with anesthesia. Correct reporting depends on who sedates and who scans, and the answer changed meaningfully in 2017.
Cardiologist performs the TEE and directs moderate sedation
Before 2017, sedation was built into the TEE codes through CPT’s Appendix G. Effective January 1, 2017, the AMA deleted the old sedation codes (99143 through 99150), removed Appendix G, and created 99151 through 99157 so sedation could be reported on its own line. A cardiologist sedating an adult for a TEE reports 99152 for the first 15 minutes of intraservice time (a minimum of 10 documented minutes, with an independent trained observer monitoring the patient) and +99153 for each additional 15 minutes. One warning before assuming payment: NGS article A52868 still instructs that sedation is included in codes 93312 through 93318 and will be bundled if billed. When the CPT book and a Medicare contractor disagree, the contractor’s edit decides the remittance.
Anesthesia professional sedates while another physician scans
The anesthesia claim uses a crosswalked anesthesia code, not the TEE code. The ASA Crosswalk directs anesthesia for a TEE performed by another physician to 01922, anesthesia for noninvasive imaging, at 7 base units. When a TEE and a cardioversion share one anesthetic, only one anesthesia code goes on the claim, and 01922 outranks 00410 (electrical conversion of arrhythmias, 4 base units) because the higher base value governs.
Anesthesiologist personally performs a diagnostic TEE during their own case
This is billable, but only with the right training, hospital privileges, and modifiers. The ASA Statement on Transesophageal Echocardiography, updated in October 2022, instructs the anesthesiologist to append modifier 59 to the TEE code to mark it as distinct from the anesthesia service, adding modifier 26 when the facility owns the equipment. NCCI treats echocardiography as integral to anesthesia, so a claim without modifier 59 fails automatically. Monitoring-only TEE by the anesthesia provider falls under the 93318 rules above and is usually not payable.
Choosing between a TEE and TTE CPT code
Echo CPT code selection begins with the imaging window. A TTE CPT code applies when the transducer sits on the chest wall; the TEE codes apply when the probe travels down the esophagus, usually because transthoracic views were inadequate or the target (an appendage clot, a valve vegetation, a dissection flap) sits directly behind the heart.
| Study | Code | Doppler handling |
| Complete TTE | 93306 | Spectral and color flow Doppler included |
| Complete TTE without Doppler | 93307 | Add-ons allowed |
| Limited or follow-up TTE | 93308 | Add-ons allowed |
| Complete 2D TEE | 93312 | Add-ons allowed |
The Doppler logic inverts between the two families. Code 93306 already contains spectral and color flow Doppler, so appending 93320 or 93325 to it trips a hard NCCI edit. The TEE base codes describe 2D imaging only, which is why the Doppler add-ons (+93320 or +93321 for spectral, +93325 for color flow) are legitimately reported alongside 93312, 93314, 93315, or 93317.
A diagnosis-coding requirement flows from this relationship. NGS wants R93.1 or R93.8 (abnormal or inconclusive cardiac imaging) listed first when the TEE was ordered because the TTE could not visualize a structure it normally shows, with the underlying cardiac condition coded second.
Add-on codes and contrast reporting
Three-dimensional imaging has two paths. +93319, added to CPT in 2022, reports 3D acquisition and postprocessing during a TEE and attaches to base codes 93312, 93314, 93315, and 93317. Codes 76376 and 76377 report 3D rendering more broadly; 76377 requires an independent workstation, a written clinical request, and a report that answers that request, and payers deny it when 2D imaging already supplied the answer. Hospitals paid under OPPS have a separate wrinkle: when contrast is used, they report C8925 in place of 93312, C8926 for the congenital study, and C8927 for monitoring TEE.
What 2026 changed, and what it left alone
The CPT 2026 release was the largest cardiology update in years: 288 new codes, 84 deletions, and 46 revised descriptors, including a full rebuild of percutaneous coronary intervention coding and 46 new lower extremity revascularization codes (37254 through 37299), summarized in the American College of Cardiology’s December 4, 2025 Coding Corner. The TEE family was not part of it. Codes 93312 through 93318 and 93355 enter 2026 with unchanged descriptors.
Payment moved anyway. The 2026 Medicare conversion factor rose to $33.40 for most clinicians ($33.57 for qualifying APM participants) from $32.35 in 2025, while CMS applied a new 2.5 percent efficiency adjustment that lowered the work values of most procedural and imaging services. For echocardiography, the two changes largely offset each other, so flat professional reimbursement is the realistic budgeting assumption.
A working summary for TEE claims
Most TEE CPT code errors trace back to the purpose of the study rather than the digits of the code. Claims fail because a monitoring exam went out as diagnostic, a structural-guidance case went out as 93312, or a sedation line was added against a contractor policy that bundles it. The reliable sequence runs in four steps: confirm the clinical purpose (diagnostic, monitoring, or interventional guidance), match the code to the work actually performed and documented, attach Doppler and 3D add-ons only to valid base codes, and check the current quarterly NCCI edits plus your MAC’s billing article before the claim leaves the door. A2Z Billings maintains this reference for the cardiology practices, anesthesia groups, and coding students it works with, and the closing rule applies everywhere: when a payer policy and the CPT book conflict, as they still do on sedation, build the claim around the policy that will actually adjudicate it.
