
United States surgeons perform more than 270,000 appendectomies each year, according to a textbook chapter published by the Society of Laparoscopic and Robotic Surgeons, and the laparoscopic approach dominates. A 2025 multicenter analysis in the World Journal of Emergency Surgery found that over 95 percent of appendectomies have been performed laparoscopically since 2017. For coders, that volume funnels into one procedure code. The CPT code for laparoscopic appendectomy is 44970. Although the code is straightforward, claims fail in the circumstances surrounding it, such as conversions to open surgery, abscess drainage, and inadvertent removals. This guide covers the code, its open and robotic counterparts, the matching ICD-10 codes, and the 2026 payment rules.
What is the laparoscopic appendectomy CPT code?
Report CPT code 44970 for a laparoscopic appendectomy. The American Medical Association descriptor reads “Laparoscopy, surgical, appendectomy,” and the code sits in the digestive system surgery section of CPT under laparoscopic procedures on the appendix.
The code has some history. The first laparoscopic appendectomy was carried out in 1980 by German gynecologist Kurt Semm, who also reported the procedure in the journal Endoscopy in 1983. CPT originally listed the procedure as 56315 in its old laparoscopy series. The 2000 edition of CPT deleted that series and relocated laparoscopic codes into their anatomic sections, which is how 44970 came to exist.
Technique does not change the code. Three-port, single-incision, endoloop ligation, or stapled transection of the appendiceal base all map to 44970.
CPT code 44970 description
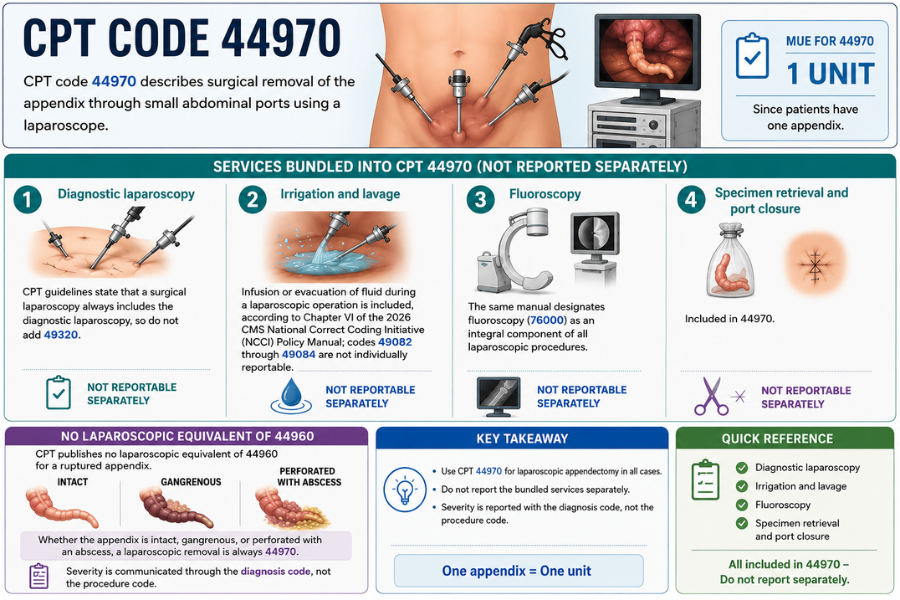
Code 44970 describes surgical removal of the appendix through small abdominal ports using a laparoscope. Several services are bundled into it and cannot be reported separately:
- Diagnostic laparoscopy. CPT guidelines state that a surgical laparoscopy always includes the diagnostic laparoscopy, so do not add 49320.
- Irrigation and lavage. Infusion or evacuation of fluid during a laparoscopic operation is included, according to Chapter VI of the 2026 CMS National Correct Coding Initiative (NCCI) Policy Manual; codes 49082 through 49084 are not individually reportable.
- Fluoroscopy. The same manual designates fluoroscopy (76000) as an integral component of all laparoscopic procedures.
- Specimen retrieval and port closure.
One point trips up coders who work from the open codes: CPT publishes no laparoscopic equivalent of 44960 for a ruptured appendix. Whether the appendix is intact, gangrenous, or perforated with an abscess, a laparoscopic removal is always 44970. Severity is communicated through the diagnosis code, not the procedure code. The Medically Unlikely Edit for 44970 is one unit, since patients have one appendix.
Open vs laparoscopic appendectomy CPT codes
The full appendectomy code family looks like this:
| CPT code | Approach | Use |
| 44950 | Open | Appendectomy, uncomplicated |
| +44955 | Open | Add-on: appendectomy for an indicated purpose during another major procedure |
| 44960 | Open | Appendectomy for widespread peritonitis or burst appendix with abscess |
| 44970 | Laparoscopic | Appendectomy, any severity |
| 44979 | Laparoscopic | Unlisted laparoscopy procedure, appendix |
Severity distinctions exist only on the open side. An open case for a perforated appendix with generalized peritonitis moves from 44950 to 44960, while the same pathology treated laparoscopically stays at 44970.
Conversion to open follows a firm rule: report only the completed open procedure (44950 or 44960), never 44970 in addition. Consulting firm KZA and AAPC’s General Surgery Coding Alert both confirm this convention, and payer edits treat the attempted laparoscopic portion as included. Append modifier 22 to the open code if the operative note documents substantial extra work from the failed laparoscopic attempt, and add ICD-10-CM code Z53.31 (laparoscopic surgical procedure converted to open procedure) as a secondary diagnosis.
Robotic appendectomy CPT code
No separate CPT code exists for a robotic appendectomy. Robotic assistance is considered a laparoscopic technique for CPT purposes, so a da Vinci or similar robot-assisted case is still reported with 44970. HCPCS code S2900 (surgical techniques requiring use of robotic surgical system) can be listed alongside it, but Medicare does not pay it and few commercial payers do.
Robotic volume remains small in emergency surgery. Only 1.6% of minimally invasive emergency general surgery procedures were carried out robotically, according to a study of the National Inpatient Sample from 2008 to 2020. On the inpatient facility side, hospitals add ICD-10-PCS code 8E0W4CZ (robotic assisted procedure of trunk region, percutaneous endoscopic approach) to capture the robot.
ICD-10 diagnosis codes for appendectomy
With effect from October 1, 2025, the FY2026 ICD-10-CM code set divides acute appendicitis into four categories: peritonitis, perforation, gangrene, and abscess. Common selections include:
| ICD-10-CM code | Description |
| K35.80 | Unspecified acute appendicitis |
| K35.200 | Acute appendicitis without an abscess or perforation, accompanied by widespread peritonitis |
| K35.201 | With generalized peritonitis and perforation, without abscess |
| K35.210 / K35.211 | With generalized peritonitis and abscess (without / with perforation) |
| K35.30 | With localized peritonitis, without perforation or gangrene |
| K35.31 | With localized peritonitis and gangrene, without perforation |
| K35.32 / K35.33 | with localized peritonitis and perforation (with or without an abscess) |
| K36 | Other appendicitis (chronic or recurrent) |
| K37 | Unspecified appendicitis |
| Z53.31 | Laparoscopic procedure converted to open (secondary only) |
Code from the operative findings and pathology report rather than the presenting symptom. A patient admitted with right lower quadrant pain (R10.31) who leaves the operating room with confirmed perforated appendicitis should carry the definitive K35 code. Specificity matters beyond the claim: the sixth character separating “with abscess” from “without abscess” affects MS-DRG assignment and severity reporting on the hospital side.
ICD-10-PCS code for laparoscopic appendectomy
Hospital inpatient coders report the procedure with ICD-10-PCS code 0DTJ4ZZ. The seven characters break down as: 0 (medical and surgical), D (gastrointestinal system), T (resection), J (appendix), 4 (percutaneous endoscopic approach), Z (no device), Z (no qualifier).
Related PCS codes include 0DTJ0ZZ for an open appendectomy and 0DBJ4ZZ when only a portion of the appendix is excised laparoscopically, since PCS reserves “resection” for removal of the entire organ. Remember the division of labor: ICD-10-PCS applies only to hospital inpatient claims, while CPT covers physician billing and outpatient facility reporting.
Global period and RVU for CPT 44970
CPT 44970 carries a 90-day global period under the Medicare Physician Fee Schedule. The global package spans the day before surgery, the day of surgery, and 90 days of routine postoperative care, including hospital visits and the wound check in clinic.
The 2026 CMS relative value file assigns 44970 a work RVU of 9.21 and total facility RVUs of 17.31, which produces a national payment of roughly $578 at the 2026 non-QP conversion factor of $33.4009 before geographic adjustment. The work RVU dropped from 9.45 in 2025 because CMS applied a 2.5 percent “efficiency adjustment” to most non-time-based procedures in the 2026 fee schedule, a change worth knowing when surgeons ask why their per-case credit shrank.
Because appendectomies are almost always urgent, the same-day evaluation that led to surgery is payable. Append modifier 57 (decision for surgery) to that E/M service; without it, payers fold the visit into the global package.
Modifiers for CPT 44970
Choose modifiers from the operative documentation and the timeline relative to the global period:
- Modifier 22: substantially increased work, such as dense adhesions or a retrocecal appendix requiring extensive dissection. Submit the operative note and expect payer review.
- Modifier 51: multiple procedures at the same session; applied to the lower-valued code. Many payers add it automatically.
- Modifier 52 or 53: reduced services, or a procedure discontinued for patient safety (for example, hemodynamic instability after induction).
- Modifier 59 or the X{EPSU} subset: a distinct procedure at a separate site during the same session, used to override an NCCI edit when documentation supports it. NCCI lists 44970 as a column 2 code under many larger laparoscopic procedures with a modifier indicator of 1.
- Modifier 78: unplanned return to the operating room during the 90-day global for a related complication, such as washout of a postoperative abscess. Medicare pays only the intraoperative portion and the global period does not reset.
- Modifier 79: an unrelated procedure during the global period.
- Modifiers 80, 82, and AS: assistant surgeon (physician) or non-physician assistant at surgery, when payer policy allows an assistant for 44970.
Modifier 50 never applies. The appendix is a single midline-adjacent organ, and the MPFS bilateral indicator for 44970 confirms bilateral billing is invalid.
Related procedures and special coding situations
Laparoscopic appendectomy with partial cecectomy. No dedicated CPT code exists for this combination. When the surgeon staples across a small cuff of cecum because the appendiceal base is inflamed, most coding advice, including discussion threads moderated on AAPC’s forums, supports reporting 44970 alone, treating the cuff as incidental to the appendectomy. A formal segmental cecal resection without anastomosis has no specific laparoscopic code, so report unlisted code 44238 (unlisted laparoscopy procedure, intestine except rectum) with a comparison code in the documentation. If the resection meets a partial colectomy descriptor with anastomosis, 44204 or 44205 (laparoscopic) or 44160 (open ileocecectomy) may apply instead.
Cecorrhaphy. Suture repair of a cecal perforation performed open is 44604; done laparoscopically, it again falls to unlisted code 44238.
Abscess drainage. Draining a periappendiceal abscess during the appendectomy is included in 44970. Standalone drainage options are 44900 for open incision and drainage of an appendiceal abscess and 49406 for image-guided percutaneous catheter drainage. A purely laparoscopic drainage of a pelvic abscess without appendectomy has no specific code; unlisted code 49329 is the common choice.
Incidental appendectomy. The 2026 NCCI Policy Manual states that removal of a normal appendix during another laparoscopic procedure is not separately reportable. When the appendix is diseased and removed for cause during another operation, report add-on code +44955 for open cases. For a laparoscopic indicated appendectomy during another laparoscopic procedure, AAPC guidance directs coders to 44970 (with modifier 59 if an edit applies) rather than +44955, which belongs to the open family.
FAQs
What is CPT code 44970?
The AMA code for a surgical laparoscopic appendectomy. It covers both ruptured and non-ruptured appendicitis and bundles the diagnostic laparoscopy, irrigation, and fluoroscopy.
What is the CPT code for appendectomy?
For open surgery, 44950 for an uncomplicated appendectomy and 44960 for a ruptured appendix with abscess or generalized peritonitis. Laparoscopic cases use 44970.
What is the ICD-10-PCS code for laparoscopic appendectomy?
0DTJ4ZZ, resection of the appendix by percutaneous endoscopic approach. Open resection is 0DTJ0ZZ..
What is the CPT code for robotic appendectomy?
Still 44970. Robot assistance is treated as laparoscopic; HCPCS S2900 may be added but Medicare does not reimburse it.
What is a partial cecectomy?
Removal of part of the cecum, usually because inflammation or perforation involves the appendiceal base. A small stapled cuff is coded within 44970; a formal laparoscopic cecal resection without anastomosis requires unlisted code 44238.
Quick reference before you bill
Confirm four things on every claim: the laparoscopic appendectomy CPT code 44970 (or the open code alone if the case converted, with Z53.31 as a secondary diagnosis), a K35-series diagnosis specific to perforation and abscess status, modifier 57 on the same-day E/M that produced the surgical decision, and no separately billed drainage, lavage, or diagnostic laparoscopy from the same session. Those four checks account for most appendectomy denials, and each one traces back to a written CMS or AMA rule rather than payer habit. Billing services that handle general surgery claims, such as A2Z Billings, typically run this same four-point check before submission rather than after a denial comes back.