A radiology order that reads “US renal complete” looks simple enough until the report reaches a coder’s desk. Does the documentation actually support CPT 76770, or does a missing structure push the claim down to 76775? Was the bladder part of the study, and does that change anything? The renal ultrasound CPT code set is small (76770, 76775, 76776, and the duplex codes that occasionally ride alongside them), but the rules for choosing between them are specific enough that one undocumented structure can change what the claim pays. This piece walks through what each code actually requires, where kidney and bladder billing gets confused with pelvic ultrasound, and which ICD-10-CM codes typically justify the exam. The distinctions matter equally for radiology billing teams and for urology revenue cycle management, since both specialties order this study constantly.
What is CPT 76770?
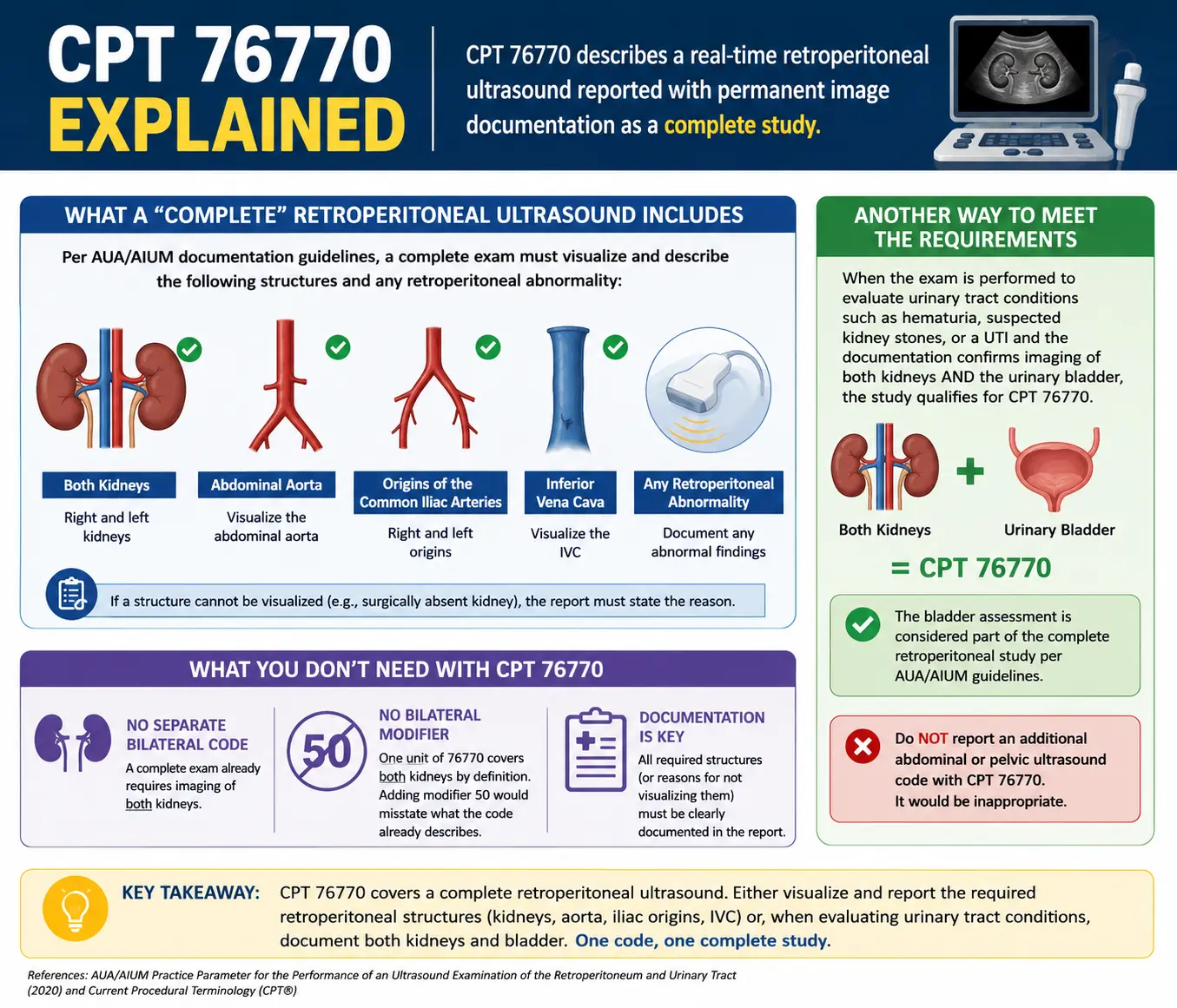
CPT 76770 describes a real-time retroperitoneal ultrasound, sometimes still called a renal sonogram in casual conversation, reported with permanent image documentation as a complete study. A joint documentation guide from the American Urological Association (AUA) and the American Institute of Ultrasound in Medicine (AIUM) defines the complete exam as scans of both kidneys, the abdominal aorta, the origins of the common iliac arteries, and the inferior vena cava, along with any retroperitoneal abnormality found along the way. Every one of those structures needs to be visualized and described in the report, or the chart needs to state why a structure could not be seen, such as a kidney that is surgically absent.
There is another, often overlooked, way to meet the requirements for a complete retroperitoneal ultrasound. When the exam is performed to evaluate urinary tract conditions such as hematuria, suspected kidney stones, or a urinary tract infection and the documentation confirms imaging of both kidneys and the urinary bladder, the study qualifies for CPT 76770. This frequently causes confusion because many coders assume that imaging the bladder requires a separate pelvic ultrasound code in addition to the retroperitoneal ultrasound. However, that is not the case. According to the AUA/AIUM Practice Parameter, when the examination follows this urinary-tract evaluation pathway, the bladder assessment is considered part of the complete retroperitoneal study. Therefore, reporting an additional abdominal or pelvic ultrasound code with CPT 76770 would be inappropriate.
Because a complete exam already requires bilateral kidneys, there is no separate bilateral renal ultrasound CPT code, and no bilateral modifier to append. One unit of 76770 covers both kidneys by definition; adding modifier 50 would misstate what the code already describes.
CPT 76775: the limited exam, and why studies get downgraded
CPT 76775 shares its descriptor with 76770 apart from one word: limited instead of complete. It applies whenever the study covers one or more, but not all, of the required elements, such as a single kidney, the aorta alone, or a bladder-only view that does not also cover both kidneys. It is also the correct code for a focused follow-up on a single previously identified finding, like rechecking one hydronephrotic kidney rather than re-imaging the entire retroperitoneum.
Downgrades from 76770 to 76775 happen more often than most practices would like, and the cause is almost always documentation rather than technique. A sonographer might capture every required structure, but if the interpreting physician’s report never mentions the inferior vena cava, and never explains why, the study can only support the limited code. AIUM’s practice parameter for ultrasound documentation puts it directly: there should be a permanent record of the examination and its interpretation, with every anatomic area imaged described in a written report. A study that was technically complete but incompletely dictated becomes, for coding purposes, a limited study.
76770 vs 76775 at a glance
| CPT 76770 (complete) | CPT 76775 (limited) | |
| Required elements | Both kidneys, aorta, common iliac artery origins, IVC (or kidneys plus bladder for urinary tract pathology) | One or more elements from the complete list, but not all |
| Typical use | Initial retroperitoneal workup, AAA screening with renal views, hematuria workup covering kidneys and bladder | Single-kidney follow-up, aorta-only recheck, bladder-only view |
| Documentation standard | Every required structure described, or a stated reason for omission | Focused description limited to the structure or structures actually imaged |
CPT 76776: why a transplanted kidney gets its own code
A native kidney sits in the retroperitoneum. A transplanted one does not. Surgeons place a donor kidney in the iliac fossa and connect it to the iliac vessels, while the native kidneys and their original vasculature are usually left undisturbed. Because the graft is not retroperitoneal tissue, 76770 and 76775 do not describe it. CPT assigns a separate code, 76776, defined as an ultrasound of a transplanted kidney performed with both real-time imaging and duplex Doppler.
That pairing, grayscale imaging plus Doppler combined into a single code, is what sets 76776 apart from the rest of the renal ultrasound CPT code family. Standard transplant surveillance calls for exactly this combination: B-mode measurements of the graft alongside resistive index calculations from the intrarenal arteries, since a rising resistive index can be an early signal of rejection or obstruction. If a transplant study is performed without any Doppler component, which is uncommon in current practice, the closer applicable code becomes 76775, since duplex Doppler is a required part of 76776 by definition rather than an optional add-on.
Renal artery duplex and Doppler: CPT 93975 and 93976
Everything described so far is B-scan ultrasound: grayscale, real-time anatomical imaging, without duplex Doppler. That distinction matters, because renal artery evaluation is a genuinely different service. When the clinical question shifts to blood flow (renovascular hypertension, suspected renal artery stenosis, or graft perfusion outside the transplant-specific code) the applicable codes come from the vascular duplex family instead. CPT 93975 covers a complete duplex scan of arterial inflow and venous outflow of the abdominal, pelvic, scrotal, or retroperitoneal organs, and CPT 93976 covers the same study when the scope is limited. Both require true duplex technique: color flow imaging combined with spectral Doppler waveform analysis, not a brief color overlay added just to confirm that a structure is a blood vessel.
The Medicare National Correct Coding Initiative addresses what happens when a B-scan ultrasound and a duplex study are performed at the same session. Per the NCCI Policy Manual, abdominal ultrasound codes (76700 through 76775) and abdominal duplex codes (93975, 93976) are generally performed for different clinical reasons, though there are cases where both are medically necessary and separately documented. In that case, the ultrasound code needs an NCCI-associated modifier, usually 59 or one of the more specific X-modifiers (XE, XP, XS, XU). Quarterly NCCI updates have flagged 76700, 76705, 76770, and 76775 as column-two codes against the duplex family specifically, so billing both without a modifier, or without documentation that separately justifies each service, tends to end in denial.
Where bladder ultrasound and “KUB” fit in
KUB is one of the more misleading abbreviations in urinary imaging. In its original and still most common radiology usage, KUB refers to a plain X-ray of the kidneys, ureters, and bladder, not an ultrasound at all. Patients, and occasionally referring clinicians, use “KUB ultrasound” loosely to mean any sonographic look at the urinary tract, but no CPT code is actually called a KUB ultrasound. Billing still depends entirely on which structures were imaged and why.
If only the bladder is evaluated in real time, without the kidneys, that maps to CPT 76857, the limited or follow-up pelvic ultrasound code, not to 76770. The AUA/AIUM documentation guide is direct about this: bladder-only imaging should not be billed under 76770. If the study is a straightforward post-void residual measurement using a non-imaging bladder scanner rather than a full diagnostic ultrasound, the correct code is 51798 instead of 76857 or 76770. Mixing these up, billing a pelvic imaging code for what was really a bladder-volume check, or the reverse, is a recurring source of denials in urology practices that run frequent PVR checks alongside renal ultrasounds.
ICD-10 codes that support medical necessity
A renal ultrasound CPT code is only paid alongside a diagnosis code that supports medical necessity, and the correct ICD-10-CM code depends on why the exam was ordered. A few categories come up repeatedly on retroperitoneal ultrasound orders.
| Clinical indication | Common ICD-10-CM code | Notes |
| Hematuria, unspecified | R31.9 | Default symptom-level code before a cause is confirmed; more specific subcodes exist for gross versus microscopic hematuria |
| Hydronephrosis, unspecified | N13.30 | More specific N13 subcodes apply once a cause, such as a stone, is identified |
| Acquired renal cyst | N28.1 | Used once imaging confirms a non-neoplastic, acquired cyst |
| Abnormal kidney imaging finding | R93.421 / R93.422 / R93.429 | Right, left, or unspecified kidney; used for an incidentally found renal mass or finding pending further workup |
Once a definitive diagnosis is confirmed (a stone at a specific location, a staged malignancy, a named congenital anomaly) the symptom code typically gives way to the more specific one. R31.9 in particular gets overused. The R31 category includes more precise subcodes distinguishing gross from microscopic hematuria, and defaulting to the unspecified code when a more precise one is documented is a coding quality issue that payer audits do catch.
Modifiers, bundling, and the denials that follow
Two modifiers carry most of the weight in renal ultrasound billing. Modifier 26 reports the professional component: the interpreting physician’s reading and written report. Modifier TC reports the technical component: the equipment, supplies, and staff time behind image acquisition. When the same provider owns the equipment and performs the interpretation, the code is billed globally, without either modifier. When a hospital owns the scanner and an outside radiologist reads the study, the hospital bills TC and the radiologist bills 26 on a separate claim.
An imaging study and an office visit on the same day are billed separately too. CPT’s own evaluation and management guidelines note that performing or interpreting a diagnostic test ordered during a patient encounter is not included in the E&M level; the interpretation can be reported on its own, with modifier 26 attached, as long as it produces a separate, distinctly identifiable written report. Some payers also tie reimbursement for urology ultrasound codes to facility accreditation, requiring a practice to hold current accreditation before certain codes are paid at all, so it is worth confirming accreditation status with each payer directly rather than assuming it carries over from one contract to the next.
Bundling denials are the other recurring headache. When a payer decides that two billed services should have been reported as one, the claim typically comes back with a CO-97 remark code, meaning the benefit for that service is included in the payment for another procedure already adjudicated. CMS has described modifier 59 as a modifier of last resort, meant to be used only when no more specific X-modifier fits, and the Office of Inspector General has recommended that CMS run pre- and post-payment reviews on claims that carry it. None of that makes the modifier something to avoid. It means the record has to show a genuinely separate session, a separate anatomic site, or a distinct medical reason for each service billed, since NCCI edits get revised every quarter and a code pair that was billable together last year may not be this year.
Getting the report right the first time
Most of what separates a clean 76770 claim from a downcoded 76775, or a paid duplex study from a denied one, comes down to what actually made it into the written report. Every structure the CPT descriptor requires has to be named, measured where relevant, or explained if it was skipped. A coder reading a renal ultrasound order still has to reconcile three things: the reason the study was ordered, the images that were actually captured, and the language the interpreting physician chose to put in the final report. Choosing the right renal ultrasound CPT code, in the end, has less to do with memorizing a list of numbers than with matching the report to what each code was written to require.