The code numbers barely moved on January 1, 2026. The payment behind them did. Every practice that bills a cystoscopy CPT code is now working with two Medicare conversion factors, a new efficiency adjustment that trimmed work RVUs on almost every procedural code, and a reallocation of practice expense that cut facility payment while nudging office payment up. Coders who only check the descriptor will still get the code right and the revenue wrong.
This guide covers what 52000 does and does not include, how the 2026 rates shifted, the bundling rules that generate most cystoscopy denials, and how the diagnosis side of the claim needs to line up.
What CPT code 52000 covers, and what it quietly excludes
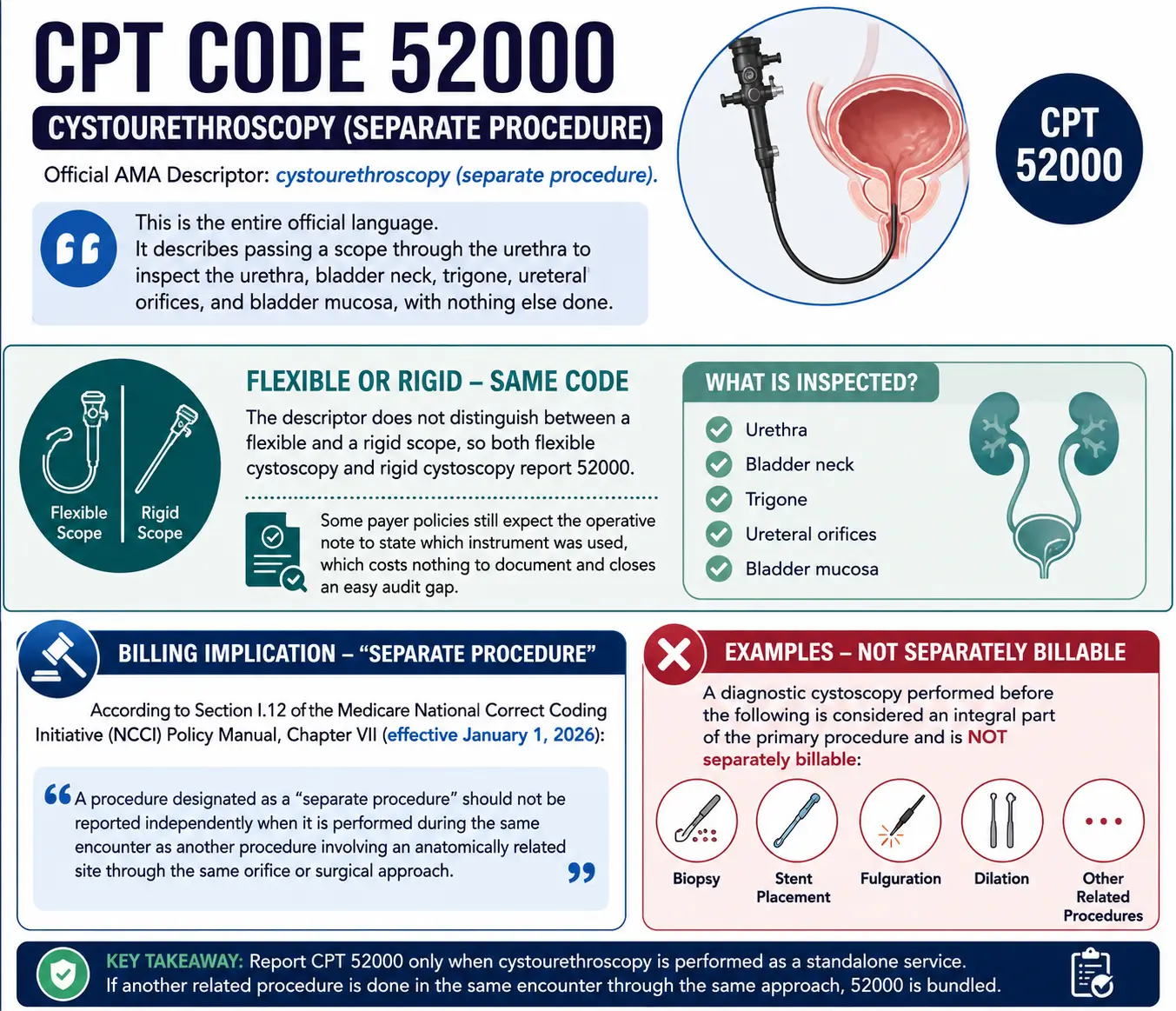
The American Medical Association descriptor for CPT code 52000 is short: cystourethroscopy (separate procedure). That is the entire official language. It describes passing a scope through the urethra to inspect the urethra, bladder neck, trigone, ureteral orifices, and bladder mucosa, with nothing else done.
The descriptor does not distinguish between a flexible and a rigid scope, so flexible cystoscopy CPT code and rigid cystoscopy both report 52000. Some payer policies still expect the operative note to state which instrument was used, which costs nothing to document and closes an easy audit gap.
The phrase in parentheses has important billing implications. According to Section I.12 of the Medicare National Correct Coding Initiative (NCCI) Policy Manual, Chapter VII (effective January 1, 2026), a procedure designated as a “separate procedure” should not be reported independently when it is performed during the same encounter as another procedure involving an anatomically related site through the same orifice or surgical approach. For example, a diagnostic cystoscopy performed before a biopsy, stent placement, fulguration, or dilation is considered an integral part of the primary procedure and is not separately billable.
What changed for the cystoscopy CPT code set in 2026
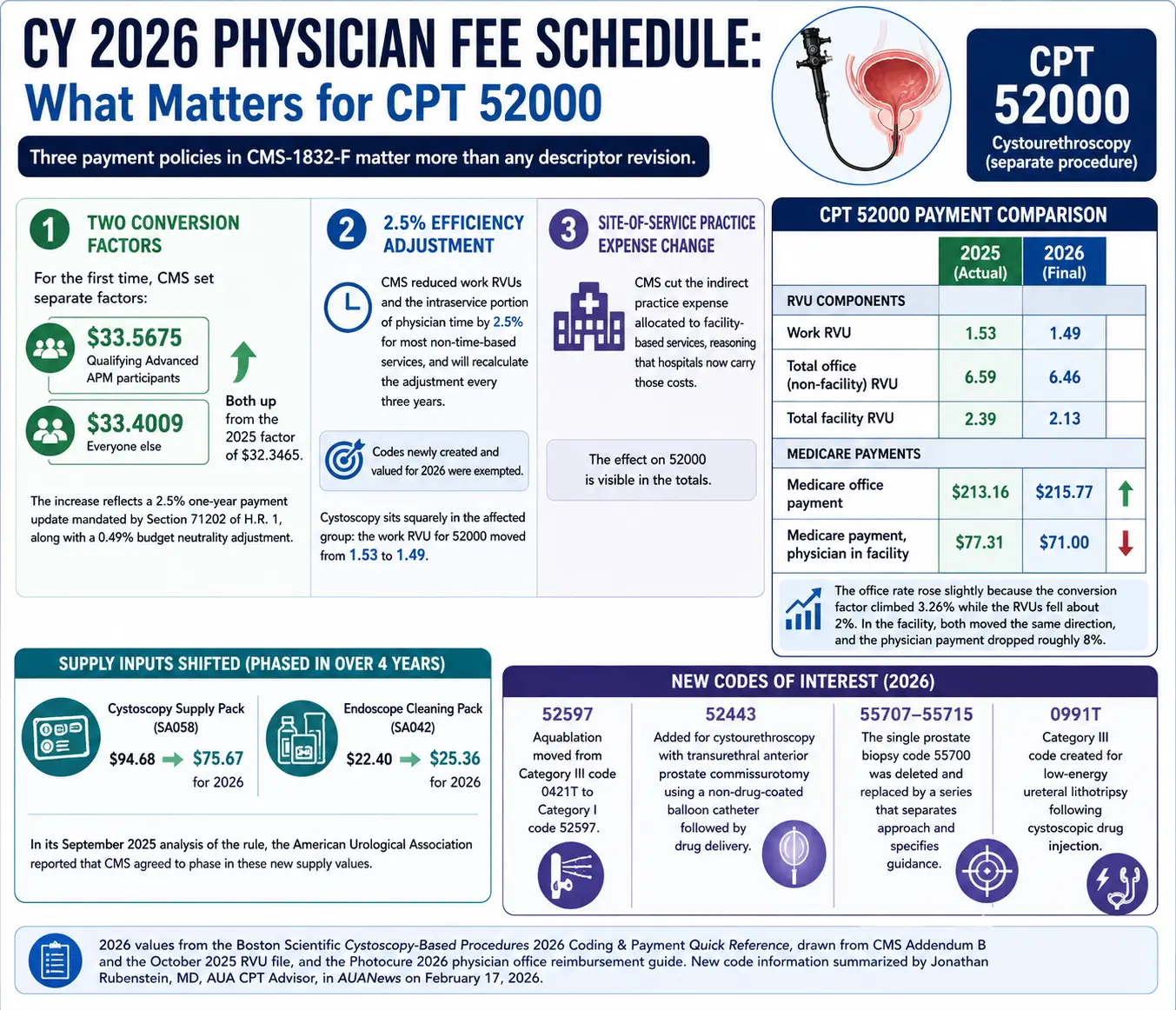
Three payment policies in the CY 2026 Physician Fee Schedule final rule (CMS-1832-F) matter more than any descriptor revision.
Two conversion factors. For the first time, CMS set separate factors: $33.5675 for qualifying Advanced APM participants and $33.4009 for everyone else, both up from the 2025 factor of $32.3465. The increase reflects a 2.5% one-year payment update mandated by Section 71202 of H.R. 1, along with a 0.49% budget neutrality adjustment.
A 2.5 percent efficiency adjustment. CMS reduced work RVUs and the intraservice portion of physician time by 2.5 percent for most non-time-based services, and will recalculate the adjustment every three years. Codes newly created and valued for 2026 were exempted. Cystoscopy sits squarely in the affected group: the work RVU for 52000 moved from 1.53 to 1.49.
A site-of-service practice expense change. CMS cut the indirect practice expense allocated to facility-based services, reasoning that hospitals now carry those costs. The effect on 52000 is visible in the totals.
CPT 52000 | 2025 | 2026 |
Work RVU | 1.53 | 1.49 |
Total office (non-facility) RVU | 6.59 | 6.46 |
Total facility RVU | 2.39 | 2.13 |
Medicare office payment | $213.16 | $215.77 |
Medicare payment, physician in facility | $77.31 | $71 |
2026 values from the Boston Scientific Cystoscopy-Based Procedures 2026 Coding & Payment Quick Reference, drawn from CMS Addendum B and the October 2025 RVU file, and the Photocure 2026 physician office reimbursement guide.
The office rate rose slightly because the conversion factor climbed 3.26 percent while the RVUs fell about 2 percent. In the facility, both moved the same direction, and the physician payment dropped roughly 8 percent.
Supply inputs shifted too. In its September 2025 analysis of the rule, the American Urological Association reported that CMS agreed to phase in a lower value for the cystoscopy supply pack (SA058), which moves to $75.67 from $94.68 for 2026, while the endoscope cleaning pack (SA042) rises to $25.36 from $22.40, both over four years.
New codes of interest, summarized by Jonathan Rubenstein, MD, the AUA’s Current Procedural Terminology advisor, in AUANews on February 17, 2026: aquablation moved from Category III code 0421T to Category I code 52597; 52443 was added for cystourethroscopy with transurethral anterior prostate commissurotomy using a non-drug-coated balloon catheter followed by drug delivery; the single prostate biopsy code 55700 was deleted and replaced by a series (55707 to 55715) that separates transrectal from transperineal approaches and specifies the guidance used; and Category III code 0991T was created for low-energy ureteral lithotripsy following cystoscopic drug injection.
Choosing the right cystourethroscopy CPT code
Code selection turns on one question: what was done after the scope went in. The 2026 Medicare national averages below come from the Boston Scientific guide cited above.
Code | Service | Office | Physician in facility |
52000 | Cystourethroscopy (separate procedure) | $216 | $71 |
52001 | With irrigation and evacuation of multiple obstructing blood clots | $420 | $253 |
52005 | With ureteral catheterization, exclusive of radiologic service | $281 | $120 |
52204 | With biopsy(s) | $355 | $127 |
52224 | With fulguration or treatment of MINOR lesion(s) under 0.5 cm | $761 | $176 |
52234 | Removal of small bladder tumor(s) measuring 0.5–2.0 cm. | N/A | $217 |
52235 | Resection of MEDIUM bladder tumor(s), 2.0 to 5.0 cm | N/A | $255 |
52240 | Resection of LARGE bladder tumor(s), over 5.0 cm | N/A | $344 |
52260 | Bladder dilation for interstitial cystitis, general or spinal anesthesia | N/A | $186 |
52265 | Bladder dilation for interstitial cystitis, local anesthesia | $346 | $144 |
52281 | Calibration and/or dilation of urethral stricture | $311 | $137 |
52287 | Injection(s) for chemodenervation of the bladder | $364 | $149 |
52310 | Removal of foreign body, calculus, or ureteral stent; simple | $299 | $135 |
52317 | Litholapaxy, simple or small (under 2.5 cm) | $869 | $304 |
52332 | Insertion of indwelling ureteral stent | $373 | $140 |
An “N/A” designation means Medicare has not assigned a payment value for the procedure in the office setting. For bladder tumor resection codes, two key sizing rules apply: report the code based on the largest tumor removed, and bill only one CPT code from 52234–52240 per date of service, regardless of the number of tumors treated. This policy originates from CMS Medicare Physician Fee Schedule transmittal guidance and continues to be enforced through current payer billing edits.
Setting changes the arithmetic more than most coders expect. The same 52000 pays $216 in the office, $71 to the physician working in a facility, $311 to an ambulatory surgery center, and $712 to a hospital outpatient department under APC 5372 in 2026.
The bundling rules behind most cystoscopy denials
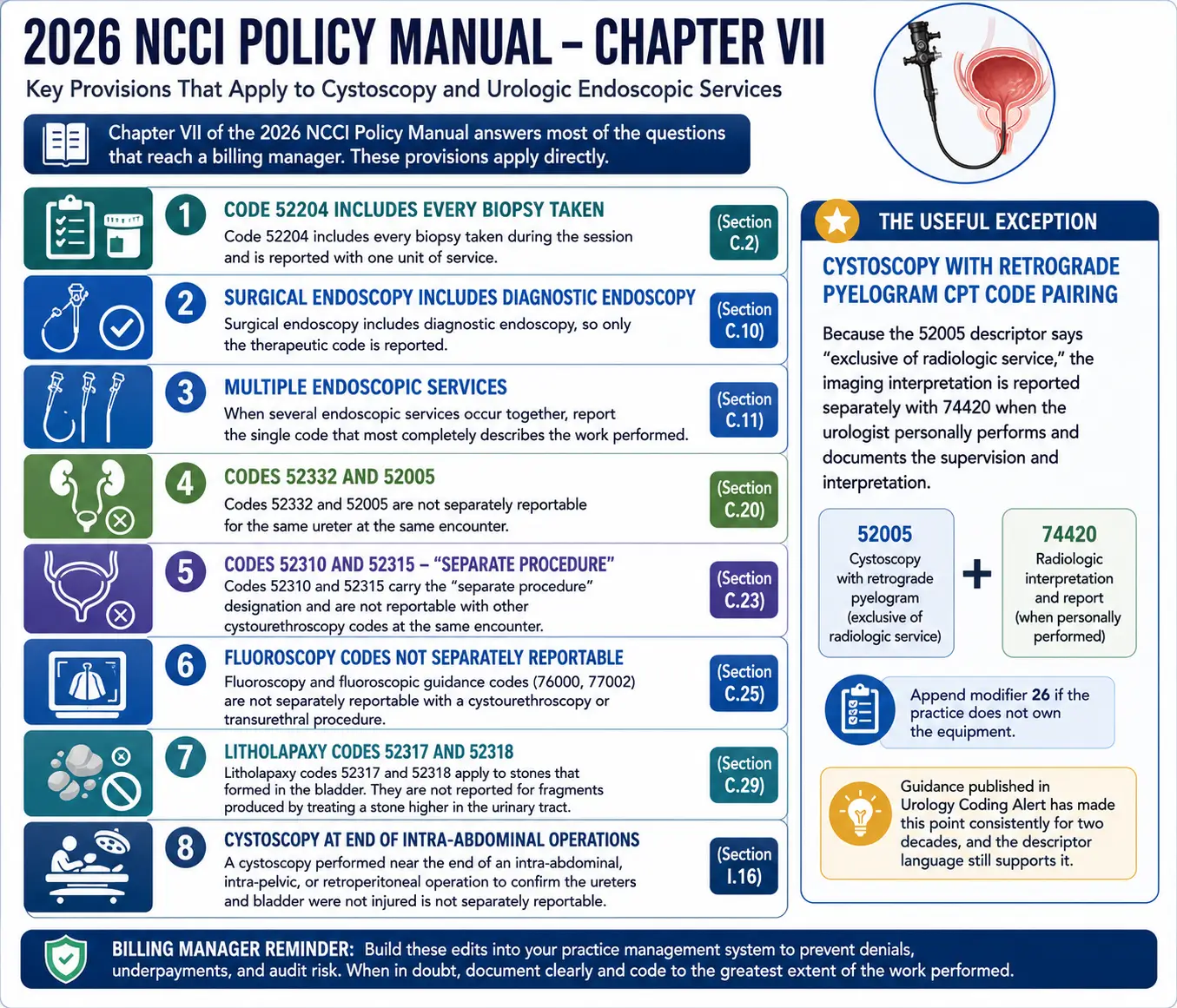
Chapter VII of the 2026 NCCI Policy Manual answers most of the questions that reach a billing manager. Several provisions apply directly:
- Code 52204 includes every biopsy taken during the session and is reported with one unit of service (Section C.2).
- Surgical endoscopy includes diagnostic endoscopy, so only the therapeutic code is reported (C.10). When several endoscopic services occur together, report the single code that most completely describes the work performed (C.11).
- Codes 52332 and 52005 are not separately reportable for the same ureter at the same encounter (C.20).
- Codes 52310 and 52315 carry the “separate procedure” designation and are not reportable with other cystourethroscopy codes at the same encounter (C.23).
- Fluoroscopy and fluoroscopic guidance codes (76000, 77002) are not separately reportable with a cystourethroscopy or transurethral procedure (C.25).
- Litholapaxy codes 52317 and 52318 apply to stones that formed in the bladder. They are not reported for fragments produced by treating a stone higher in the urinary tract (C.29).
- A cystoscopy performed near the end of an intra-abdominal, intra-pelvic, or retroperitoneal operation to confirm the ureters and bladder were not injured is not separately reportable (Section I.16). This one is billed incorrectly often enough to be worth a standing edit in the practice management system.
The cystoscopy with retrograde pyelogram CPT code pairing is the useful exception. Because the 52005 descriptor says “exclusive of radiologic service,” the imaging interpretation is reported separately with 74420 when the urologist personally performs and documents the supervision and interpretation, with modifier 26 appended if the practice does not own the equipment. Guidance published in Urology Coding Alert has made this point consistently for two decades, and the descriptor language still supports it.
Global periods and modifier decisions
The cystourethroscopy codes carry 0-day global periods in the Medicare Physician Fee Schedule relative value file, including 52000, 52204, 52332, and the tumor resection family. Transurethral prostate surgery is the contrast worth knowing: 52601 carries a 90-day global. That difference decides whether modifiers 58, 78, and 79 enter the picture at all when a patient returns.
With a 0-day global, an evaluation and management service on the same date is payable only when it is significant and separately identifiable from the work already built into the procedure, reported with modifier 25. The decision to perform the procedure does not qualify, and a new patient status by itself does not qualify either.
Laterality deserves attention. Code 52332 is unilateral, so bilateral stent placement takes modifier 50 or the RT and LT modifiers depending on the setting. Code 52287 carries a bilateral indicator of 0, meaning modifier 50 should never be appended. For stone destruction or removal, the unit of service is one per ureter regardless of the number of stones, and a bilateral procedure is reported with modifier 50 and one unit.
Stent placement, exchange, and removal
The cystoscopy with ureteral stent placement CPT code is 52332, defined as insertion of a self-retaining indwelling stent such as a double-J. Insertion and removal of a temporary ureteral catheter during a diagnostic or therapeutic procedure is not 52332 and is not separately reportable.
For a cystoscopy stent exchange CPT code, report 52332 alone. The removal is bundled by the “separate procedure” rule attached to 52310. When a stent is removed at a later encounter with no replacement, 52310 (simple) or 52315 (complicated) applies. If the stent has an external string and comes out without a scope, no cystoscopy code is billed at all; that work belongs to the E/M service.
CPT instructs that 52332 not be reported with 52353 on the same side. Lithotripsy with stent placement on the same side is 52356.
Blue light cystoscopy, drugs, and facility-only codes
There is no separate physician CPT code for blue light cystoscopy. Per Photocure’s 2026 physician office reimbursement guide, the physician reports the appropriate cystoscopy code (52000, 52204, 52214, or 52224) plus HCPCS A9589 for hexaminolevulinate hydrochloride on its own claim line, paid under average sales price methodology. Facilities use different codes: C7554 replaces 52000 and C7550 replaces 52204 in the hospital outpatient and ASC settings, with C9738 reported for other procedures.
The cystoscopy with Botox injection CPT code is 52287, paired with J0585 for the drug when the practice buys it. J0585 is defined per one unit, so a 100-unit bladder dose is 100 units on the claim, not one. Underbilling this line is a quiet, repeatable revenue loss. Single-dose vial rules still apply: report discarded amount on a separate line with modifier JW, or attest to no waste with modifier JZ.
ICD-10 coding for cystoscopy
There is no ICD-10-CM code for cystoscopy, because ICD-10-CM classifies diagnoses, not procedures. What the claim needs is a diagnosis that supports medical necessity: hematuria (R31.0, R31.1, R31.9), recurrent urinary tract infection (N39.0), bladder malignancy (C67.-), personal history of bladder cancer (Z85.51), or overactive bladder (N32.81) for chemodenervation.
Inpatient facility coders use ICD-10-PCS. Diagnostic cystoscopy is 0TJB8ZZ, inspection of bladder, via natural or artificial opening endoscopic. Ureteral stent placement is coded as dilation with an intraluminal device, 0T768DZ on the right and 0T778DZ on the left. Stent removal is 0TP98DZ, per the correction AHA Coding Clinic published to its Second Quarter 2016 advice. PCS guidelines direct that inspection is not coded separately when another root operation is performed on the same body part through the same approach.
Medical necessity rules changed on the clinical side more than the coding side. The AUA/SUFU microhematuria guideline amendment (Barocas DA, Lotan Y, Matulewicz RS, et al. Journal of Urology. 2025;213(5):547-557) recommends cystoscopy for intermediate- and high-risk patients, repeat urinalysis within six months instead of immediate cystoscopy for low or negligible risk, and reclassifies women under 60 without other risk factors as low or negligible risk rather than high risk by age alone. Documentation that names the risk tier gives a reviewer the reason the scope was indicated.
The demand for cystoscopy is expected to remain strong. According to the American Cancer Society’s Cancer Facts & Figures 2026, released on January 13, 2026, an estimated 84,530 new cases of bladder cancer and 17,870 related deaths will occur in the United States this year. Because surveillance cystoscopy is a standard component of follow-up care for most patients with bladder cancer, procedure volume is expected to remain consistently high.
Before the claim goes out
Four checks catch most of the money. Confirm that no therapeutic work is buried in the body of a note billed as 52000. Confirm the tumor measurement in the record matches the size band in the code. Confirm the drug line and its units are present on Botox and blue light claims. Confirm the place of service matches where the work happened, since the same cystoscopy CPT code carries four different Medicare amounts depending on setting.
The 2026 CPT code descriptors remain largely unchanged from 2025, but the payment values tell a different story. Work RVUs decreased by 2.5% for most procedural codes, facility practice expense values were reduced, and the Medicare conversion factor was divided into two separate rates. Practices that compare their highest-volume cystoscopy codes against the 2026 Medicare Physician Fee Schedule, rather than relying on prior-year reimbursement, will be better equipped to identify which services remain financially viable in the office setting and which may not.